As time draws near for the annual celebration of Cancer Awareness (in the month of October), data in a new Lancet Commission on Women, Power, and Cancer (LCWPC) and an accompanying analysis of previous International Agency for Research on Cancer data has shown that nearly seven in 10 women who died prematurely from cancer in 2020 could have been saved.
The research found that of the 5.3 million adults who died early from cancer last year, 2.3 million were women, with one-third killed due to a lack of timely treatment rather than prevention.
The new population-based study has estimated premature deaths from cancer at ages 30 to 69 years across 185 countries. The study looks at the preventable and treatable deaths on 36 different types of cancer. Of the estimated global cancer burden of 265.6 million years of life lost (YLLs), 182.8 million were due to premature deaths from cancer in 2020. This is equivalent to 68.8% of the total YLLs from cancer. Of these premature deaths, 124.3 million (68%) were preventable and 58.5 million (32%) were treatable.
 According to the study, lung cancer was the leading contributor to preventable premature YLLs in medium to very high human development index (HDI) countries, while cervical cancer led in low HDI countries. Colorectal and breast cancers were major treatable cancers across all four tiers of HDI. The study highlighted the need for tailored programmes of early diagnosis and screening linked to comprehensive treatment, as well as greater investment in risk factor reduction and vaccination to address premature cancer inequalities.
According to the study, lung cancer was the leading contributor to preventable premature YLLs in medium to very high human development index (HDI) countries, while cervical cancer led in low HDI countries. Colorectal and breast cancers were major treatable cancers across all four tiers of HDI. The study highlighted the need for tailored programmes of early diagnosis and screening linked to comprehensive treatment, as well as greater investment in risk factor reduction and vaccination to address premature cancer inequalities.
Further, the research showed that the interactions between women and cancer are complex and multifaceted, including participation in prevention and screening, diagnosis and treatment, caregiving, advocacy, research, and policy making.
It was also pointed out that women face structural marginalization due to gender bias and discrimination based on age, race, ethnicity, socio-economic status, sexual orientation, and gender identity, which can impede their ability to seek diagnosis and quality care. Since, cancer is a leading cause of premature mortality among women globally, the article highlighted the urgent need for more research to better understand the causes of cancer in women. Added to this, it said women also experience financial catastrophe due to cancer, and the unpaid caregiving workforce for cancer is predominantly female.
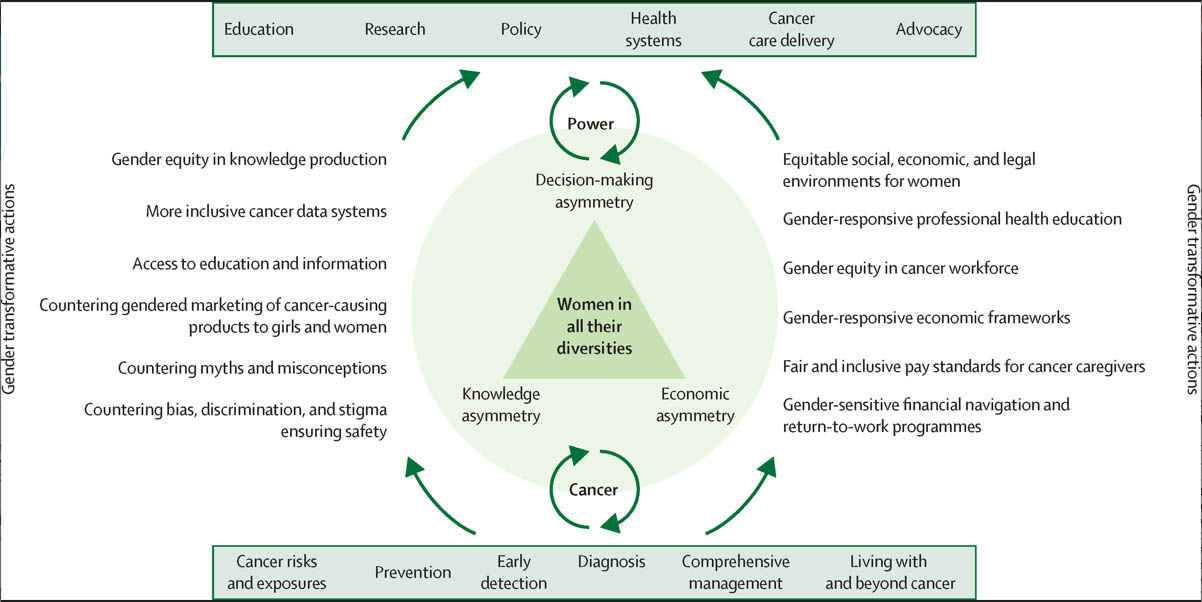 The report recommended a set of ten actions, including making all policies responsive to the needs and aspirations of women in all their diversities, and creating awareness, ensuring equitable access to research opportunities and resources, and implementing policies mandating that sex and gender dimensions are considered in research and research policy making to address gender bias and discrimination in cancer research and knowledge production. Measures are also recommended to recognize and value the unpaid caregiving work done by women in cancer care.
The report recommended a set of ten actions, including making all policies responsive to the needs and aspirations of women in all their diversities, and creating awareness, ensuring equitable access to research opportunities and resources, and implementing policies mandating that sex and gender dimensions are considered in research and research policy making to address gender bias and discrimination in cancer research and knowledge production. Measures are also recommended to recognize and value the unpaid caregiving work done by women in cancer care.
The report further highlighted overlapping forms of discrimination experienced by women from different communities and contexts in their interactions with the cancer health system. As such researchers aim to transform the way women interact with the cancer health system, whether as patients, care providers, or both.
The research acknowledged the rise in cancer cases and deaths amongst women globally, projecting a 44% increase in new cases by 2040. While wealthier economies have a higher lifetime risk of cancer, the risk of dying from cancer is similar globally, regardless of where a woman lives. Cancer health disparities largely reflect social inequalities between and within countries, driven by structural determinants such as sexism, racism, and ageism.
Intersectional
It is also understood that the commission adopts an intersectional feminist framework for cancer, challenging patriarchy and colonialism and drawing from existing feminist theories and intersectional frameworks. The report presented a global exposition of key cancer statistics in women and highlighted the disproportionately high burden of premature cancer deaths in lower human development index (HDI) countries, with breast and cervical cancer contributing to almost half of these deaths.
The proportion of preventable and treatable premature deaths is similar regardless of a country’s Human Development Index (HDI), but the top five preventable cancer deaths differ among countries with different HDIs, the research showed. Additionally, survival rates for male and female cancer patients vary due to factors such as stage at diagnosis, delays in seeking care, and comorbidities.
Breast cancer, it said, has a high likelihood of long-term survival if detected early, but there are disparities in survival rates between countries. Childhood cancer, on the other hand, has distinct patterns of cancer types and survival rates vary greatly between countries. There are also some reports of gender disparities in childhood cancer treatment, possibly due to social discrimination.
The article also discussed the gendered aspects of cancer and its risk factors, as well as the impact of cancer on women across different age groups. It noted that women represent about two thirds of new cancer cases among young adults, aged 20-39 years. Breast, thyroid, and cervical cancer are the most common diagnoses among younger women, while breast, cervical and thyroid cancer are the most common causes of death. Meanwhile, older women face barriers accessing age-appropriate care due to poverty, disability, and economic insecurity.
As is already known, tobacco use, alcohol consumption, unhealthy diet, physical inactivity, and exposure to infections are all risk factors for cancer. Alcohol consumption is linked to several types of cancer in both men and women, with women experiencing a disproportionately higher burden of alcohol-attributable cancer in many countries. Obesity is also a major driver of cancer risk, particularly among women. Commercial interests from the alcohol and beauty industries present challenges to reducing the burden of cancer, and gender-responsive policy changes within national alcohol and cancer action strategies are imperative. As such, the research noted that addressing these could save the lives of millions of women of all ages.
Household air pollution
As is well-known by many in the health sector and those who would’ve or are experiencing it in some way, lung cancer is a leading cause of cancer deaths among women. This is particularly true in Asia and Africa, due to household air pollution and high levels of biomass exposure, the research noted. It added that women are traditionally under-represented in lung cancer screening and therapeutic trials. On this note, the article recommended that future research be undertaken to better understand the gendered drivers of lung cancer risks and outcomes for women, as well as to incorporate sex and gender dimensions into clinical trials.
Breastfeeding, it was found, is associated with a lower risk of breast cancer, but the report noted that societal structural factors must be addressed to ensure access and autonomy for those who choose to breastfeed. A feminist approach, centering the voices and experiences of women in all their diversities, is crucial for capturing and addressing gendered health inequities for social and gender justice, it advocated. The article added that gender norms affect health care differently for men, women, and people of diverse sexual orientation, gender identity, and gender expression (SOGIE), and account for much of the observed cancer inequalities and differential experiences of cancer prevention and care.
It the research paper, the importance of symptom awareness and timely cancer diagnosis, particularly in low-income and middle-income countries where cancer screening coverage remains low was also discussed. It highlighted the cultural and gender-related barriers that can impede symptom appraisal and affect decisions to seek care, such as shyness, modesty, and reliance on traditional medicines.
The need for culturally embedded interventions, improvements in education and literacy levels, and the introduction of different screening methods were also noteworthy points. Further, the role of social networks and cultural beliefs in symptom sense-making and decision-making, and the impact of cancer-related stigma on care-seeking behaviours and wellbeing was highlighted.
Gender norms and financial barriers can also act as barriers to women seeking appropriate healthcare for themselves, while physical violence and concerns for safety also impact women’s access to cancer care, the report noted. Women are often diagnosed with cancers at later stages than men, and they face longer intervals from first presentation to diagnosis, resulting in more advanced stages of cancer. Gender biases and stereotypes within healthcare institutions can result in differential health outcomes for women, with women experiencing mistreatment, disrespect, negligence, and abuse by medical staff. Women also have unmet physical, psychosocial, and palliative care needs, and thus their access to these essential services may be limited by resource constraints, physician reluctance to make early referrals, geographical and financial barriers, and gender discrimination affecting the quality of care received. Added to this, the article noted that the COVID-19 pandemic has also had a disproportionate effect on women’s access to cancer care.
According to the LCWPC article, the gender gap in leadership within the field of oncology is prevalent and varies across regions and types of organizations. Women are underrepresented in leadership roles in Asia, Africa, and Europe, while men are overrepresented in hospitals, treatment centres, and research institutes. This gender imbalance has a detrimental effect on the career trajectory of oncologists, nurses, and other allied health personnel, with women frequently reporting experiences of gender discrimination and harassment. Addressing gender disparities in cancer outcomes will require advocacy efforts to ensure the implementation of gender-responsive policies in all healthcare settings, it said.
The article also discussed gender disparities in oncology research in terms of authorship, clinical trial leadership, and research funding. While progress has been made in increasing the percentage of women in senior authorship and clinical trial leadership positions, there is still room for improvement. Gender biases have been identified in grant awards and renewals.
Furthermore, unpaid care work, including caring for those with cancer, is primarily carried out by women worldwide and represents a significant contribution to society, yet it often goes unrecognized. Women from disadvantaged backgrounds and those living in rural areas who care for loved ones with cancer may have to devote a substantial amount of time to other caregiving tasks such as cooking and cleaning, which can affect their education and employment opportunities.
The burden of unpaid caregiving on women can lead to negative consequences on their careers, financial situations, and mental health. According to the findings of the research, the estimated value of unpaid cancer caregiving in Colombia, Ghana, India, Mexico, and South Africa ranged from 0.39% to 2.53% of national health expenditure. The disproportionate contribution of unpaid work is at the heart of gender inequality and intersects with other structures of inequality such as race, disability, class, age, and sexual orientation. Caring, it noted, must be considered as a social determinant of health for women because it exerts a substantial toll on the caregiver, particularly among marginalized populations.
Also noteworthy is the fact that women from countries with low human development indices accounted for 72% of premature female cancer deaths, compared to 36% in nations with high HDIs. Around 1 million children were left motherless.
As for cancer awareness celebrations around the world in the month of October, there are several notable events that take place. The most well-known is the annual Breast Cancer Awareness Month, marked by the iconic pink ribbon symbol. Many organizations and companies support the cause by donating proceeds from products sold or hosting events to raise awareness and funds for breast cancer research.
Additionally, World Cancer Day takes place on October 4th, which aims to raise awareness about cancer prevention, detection, and treatment. Other events in October include National Liver Cancer Awareness Month and National Pancreatic Cancer Awareness Month. These events serve as opportunities to educate the public about the various types of cancer and advocate for better research, detection, and treatment options.